The Road to Recovery
How Peripheral Nerves Regenerate After Hand Transplantation
There are a lot of things to consider after receiving a hand transplant; New medications to take, a new daily routine and intensive hand therapy. For someone who has just received a hand transplant, life is very different than it was before.
Peripheral nerves (any part of the nervous system other than the brain and spinal cord) play an important role in regaining function of a donor hand. After an amputation, nerves become injured and degenerate. Once major nerves have been reattached and a hand is transplanted, nerve regeneration begins to slowly take place. The following pages tell a story of how peripheral nerves regenerate, how the donor hand is reintegrated in the brain after hand transplantation, and why rehabilitation therapy is critical to the process.
Neurons
the basic components of the nervous system

Before nerve regeneration can be understood, it is important to know the fundamental anatomy and function of a nerve cell. The nervous system is made up of billions of nerve cells called neurons. Neurons come in many different varieties depending on shape and function. The most relevant neurons, in this case, are the motor neuron and sensory neuron.
Motor neurons control muscles by sending impulses to individual muscle cells. The basic structure of a motor neuron consists of a cell body with a nucleus, dendrites that branch off of the cell body to receive signals from other neurons, an axon where impulses travel, and an axon terminal where the junction between nerve cell and muscle cell is located. In a motor pathway from the brain to a muscle, there are two motor neurons—one with its cell body located in the primary motor cortex of the brain, called an upper motor neuron, and one with its cell body in the spinal cord, called a lower motor neuron. The signal from the upper motor neuron is relayed to the muscle by the lower motor neuron and causes it to contract.

Motor neuron

Sensory neuron
Sensory neurons allow an individual to perceive information about its environment. In the hands, sensory sensations come in the form of touch, pressure, vibration, limb position, heat, cold, and pain. The makeup of a sensory neuron is very similar to that of a motor neuron.
the anatomy of a nerve
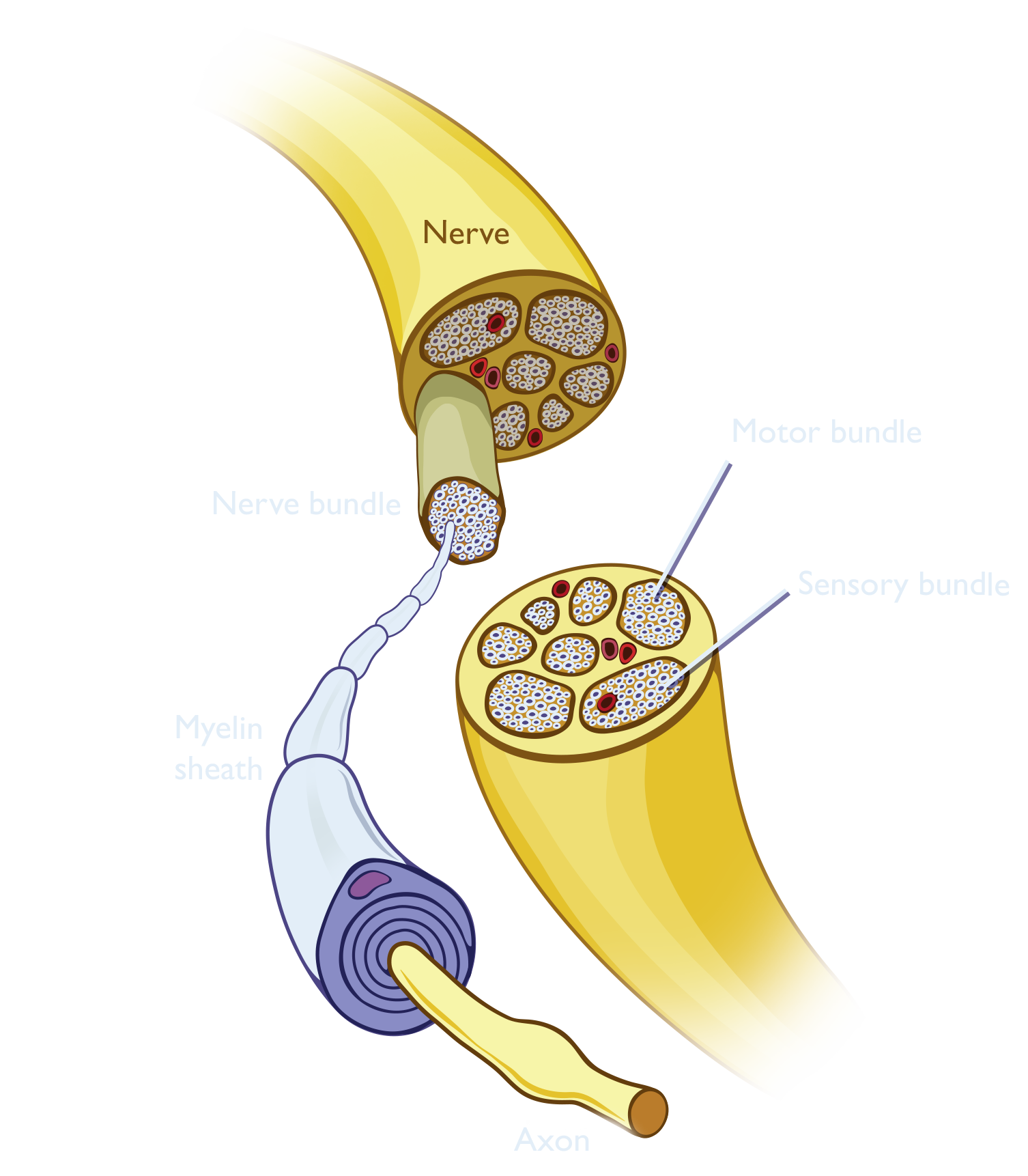
The function of an axon, or nerve fiber, is to transmit information to different cells such as other neurons or muscles. Nerve impulses travel down an axon faster if the axon is insulated by a myelin sheath. The myelin of a neuron in the peripheral nervous system is made of support cells called Schwann cells that wrap around the axon.
Axons are grouped together in bundles based on their functions, motor and sensory fibers being arranged in separate bundles. These bundles are grouped together by connective tissue to form a nerve. Both motor and sensory nerves are important to regaining critical function after a hand transplant and undergo a process of regeneration in order to regain sensory feeling and motor innervation.
Hand Transplantation & Nerve Regeneration
The transplant
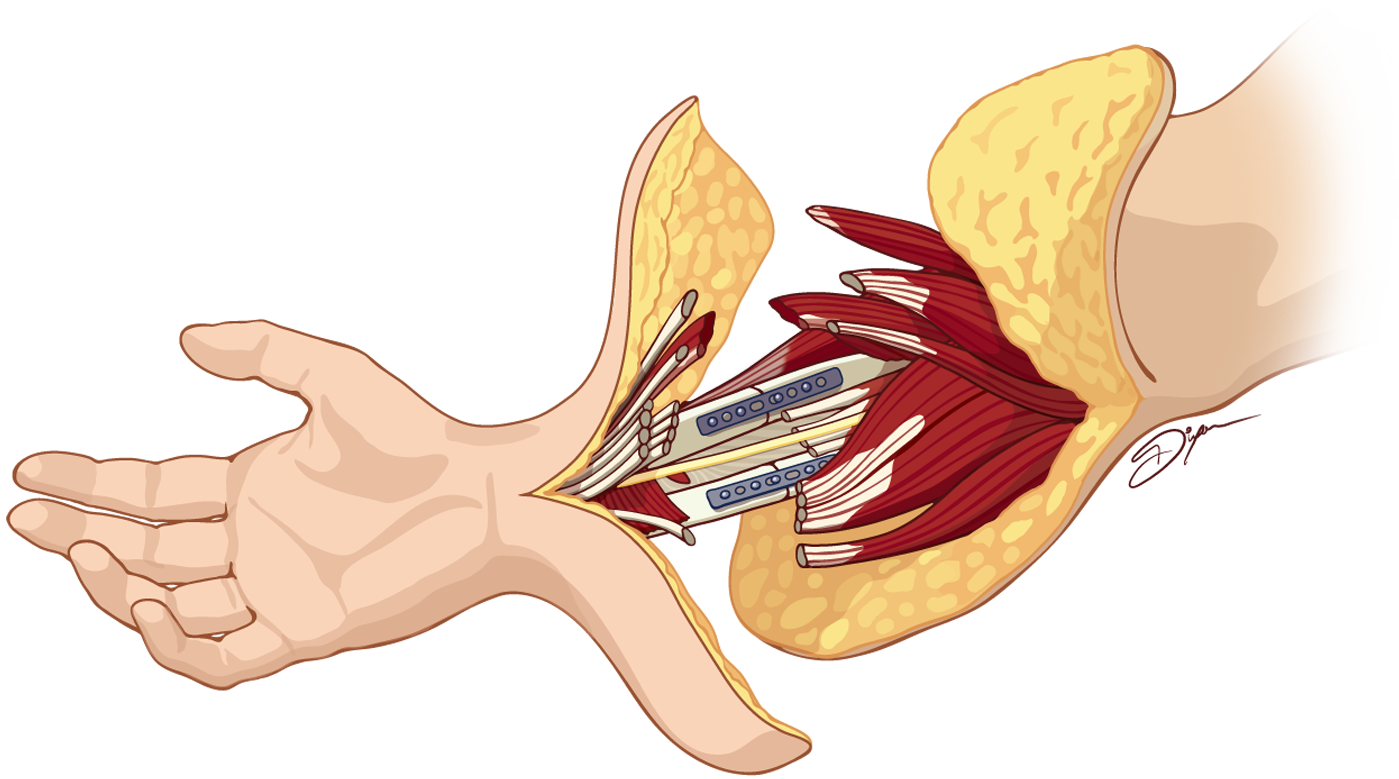
During hand transplant surgery, bone, blood vessels, muscles and tendons, nerves, and soft tissues from the donor must be attached to the recipient in a step-wise manner. First, the bones must be connected with plates and screws, after which the muscles and tendons can be attached. Veins and arteries are connected next, allowing blood to flow to the donor hand. At this stage, a recipient's nerves are connected to the nerve pathways of the donor arm. When surgeons reconnect the cut nerves with microsurgery, it must be done with care. There are distinct bundles of sensory and motor nerves, and these bundles must line up appropriately for the nerves to function properly. Finally, the remaining tissues are attached and the skin is sutured up.
After the operation, nerve regeneration, the process of growth and repair in the peripheral nervous system, must take place to regain sensation and motor function in the donor hand. Choosing to place the donor hand in the distal third of the forearm, where mostly tendons, not muscle bellies, are found is the preferred placement for optimal recovery of the hand, because nerve repair sites end up closer to the hand's target organs. Time is the currency of nerve regeneration, especially for motor nerves, as the muscle's ability to receive new nerve connections can be permanently lost if reinnervation does not occur within 12–18 months.
When nerves become injured by an amputation, they undergo a process called Wallerian degeneration. This causes a severed axon that is distal to the injury (farther from the cell body) to degenerate within 1-2 days. As soon as 1 day after injury, the proximal axon that is connected to the cell body begins regenerating as Schwann cells begin to clear the debris. A patient's nerves can grow at a rate of about 1-2mm per day, or about an inch per month, though clinical reports have noted increased rates of nerve regeneration, up to 2–3 mm per day in hand transplant patients on immune suppressive regimens and may account for the evidence of early functional recovery.
Nerve Regeneration
Peripheral nerve regeneration after hand transplantation
Peripheral nerve regeneration is the process of growth and healing in the peripheral nervous system after a nerve injury. When an axon becomes severed, the proximal segment of the host nerve, the end still attached to the cell body, begins to degenerate until Schwann cells clear cellular debris from the injury, a process that may take up to several months.
Once the debris has been cleared, the remaining axon begins to sprout smaller axonal processes. At the tip of each axon, there is a hand-like projection called a growth cone. Growth cones direct movement in the presence of chemicals, called axon guidance molecules, which attract or repel axons.
After hand transplantation, the host nerve uses the donor nerve as a scaffold to direct axon regeneration towards its muscular target. As regeneration begins along the donor nerve, host Schwann cells must migrate into the graft to support axon regeneration. Some of the donor Schwann cells may also remain and provide support.
While the nerve is repaired, degeneration of the donor nerve scaffold takes place. Fully regenerated nerves will ensure optimal functional recovery.
Cortical Reintegration
after nerve regeneration
Nerve regeneration is not the only process necessary for functional recovery. Another phenomenon called cortical reintegration, cortical reorganization, or cortical plasticity, contributes to the success of gaining function of a donor hand.
The human brain is highly plastic; it undergoes reorganization both after an amputation and a hand transplant. When a person loses a hand, the areas of the primary motor cortex and primary somatosensory cortex that were once responsible for the lost hand become reorganized to be used by other adjacent areas.
Phantom limb pain, the sensation of pain in a lost limb, is one phenomenon that can occur after significant cortical reorganization. Many forearm and hand amputees report experiencing of sensations in lost limbs, especially referred pain caused by movements of the lips. Looking at a cortical homunculus, or a visual representation of the body as it relates to areas in the motor and sensory cortices (sing. cortex), one can see that the nerve pathways of the lips are in close proximity to those that control the hands.
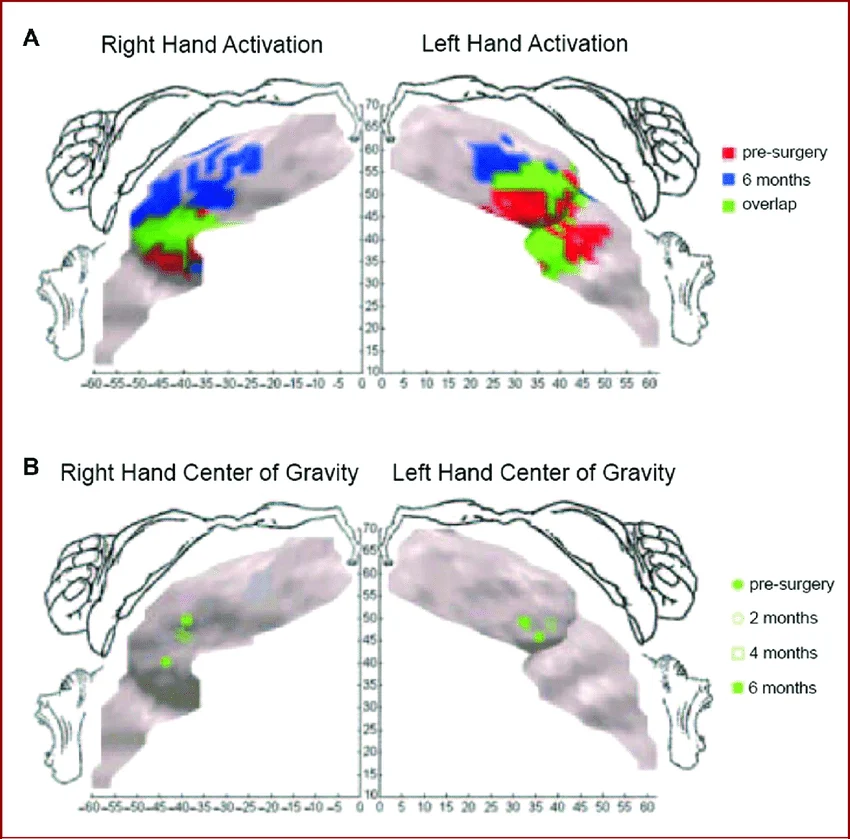
Cortical reorganization can be reversed, however, after hand transplant surgery. Research has shown that, after peripheral nerves regenerate, the pathways of the motor cortex that have reorganized themselves in response to amputation are able to return to their original orientation. This phenomenon is tested using functional magnetic resonance imaging (fMRI) and transcranial magnetic stimulation (TMS) data to map the changes in activation patterns over time. Researchers are able to measure the areas of activation in the motor cortex during imagined hand movement tasks pre-operatively and compare the results with data from actual tasks performed after transplantation. Over the course of up to 2 years, activation patterns are recorded during hand movement tasks. The regional shifts of activation areas from the same pathways in the motor cortex can be observed when comparing data sets side-by-side.
Functional Recovery with Rehabilitation
the road to recovery
Even though peripheral nerve regeneration and cortical reorganization are complex processes, they will happen naturally in the human body as long as a hand transplant patient receives the proper care and rehabilitation therapy. There are several stages of rehabilitation therapy after a hand transplant, during which several splints will be used.
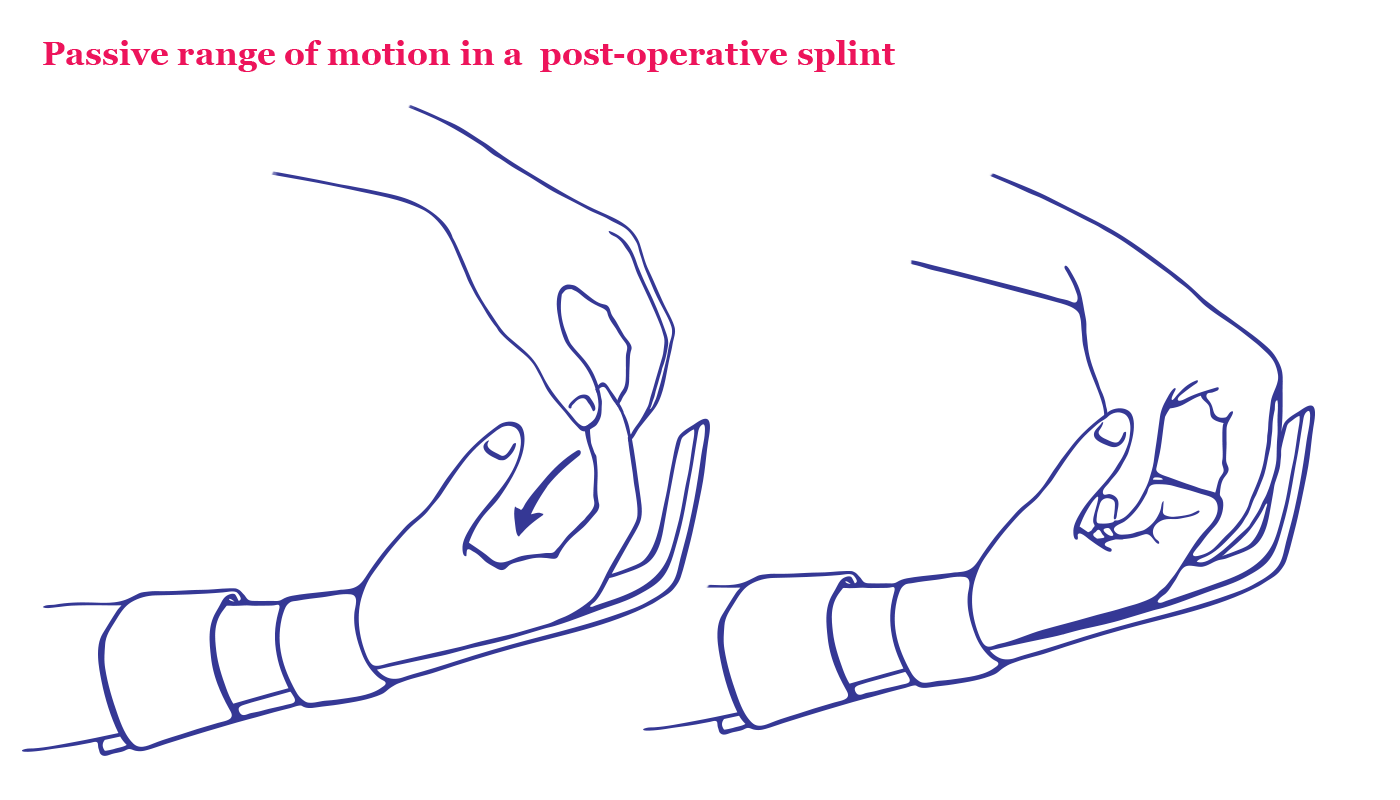
Rehabilitation therapy may begin as early as 5-7 days after a hand transplant operation. The first splint, the postoperative splint, is applied immediately after surgery. It is designed to protect tissues and properly position the limbs during healing. This splint positions the wrist in 30 degrees of extension and the metacarpo-phalangeal (MCP) joints, to be flexed at 45 degrees.

Around 5-10 days after the operation, movement exercises called early protective motion (EPM) may begin. EPM is started with a hand therapist who will work to maintain the length of the tendons and muscles in the newly transplanted hand by gently moving and stretching the fingers and wrist while the hand is unable to function. This is called passive range of motion (PROM).
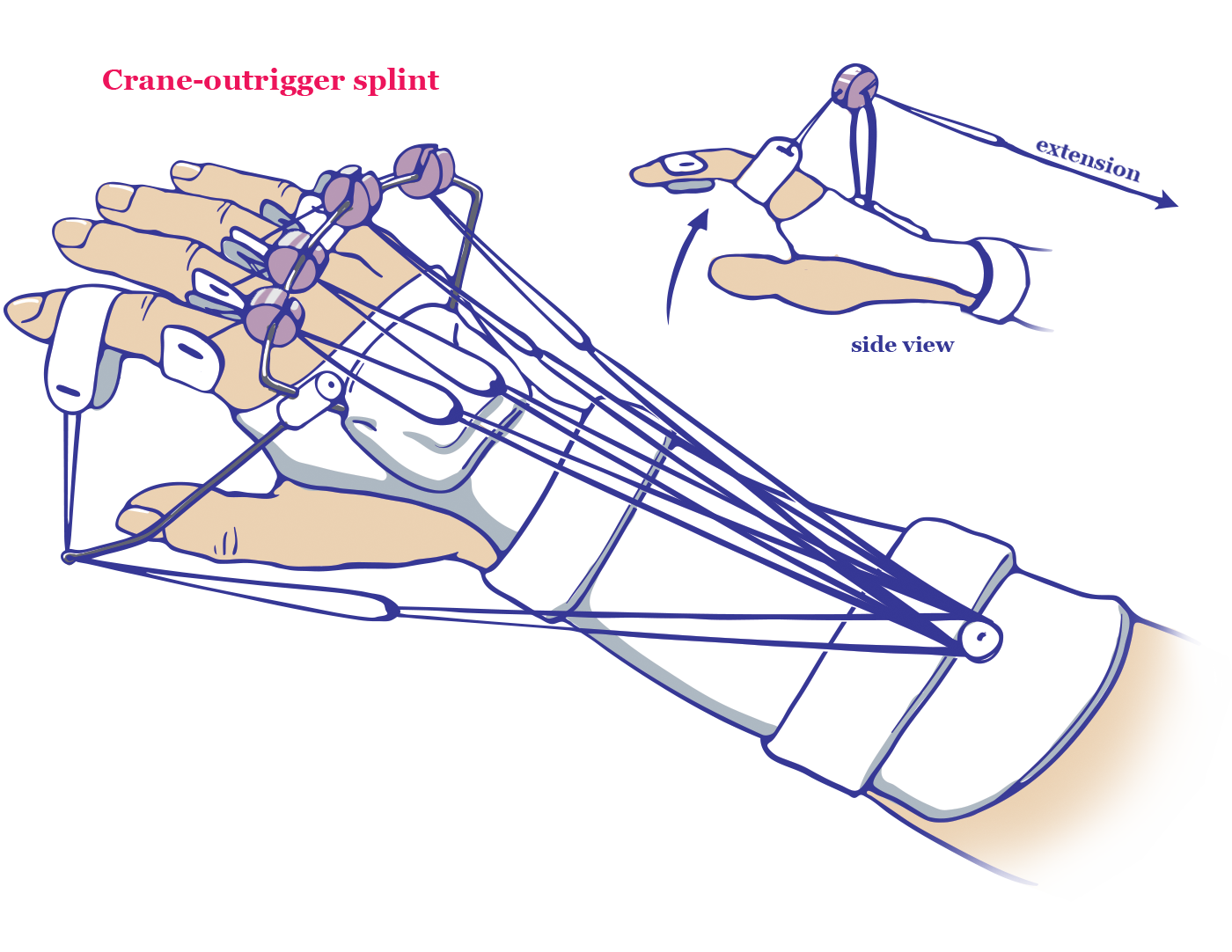
As function is recovered during nerve regeneration, the post-operative splint may be swapped for the crane-outrigger splint. This type of splint will support bones of the forearm, the radius and ulna, while protecting the extensor muscles from shortening due to a lack of use during recovery.
The last splint, the anti-claw splint, is applied 3-4 weeks post-operation. It is designed to prevent claw deformity and will be used long term until the muscles of the hand become innervated. In the beginning, it is only worn for short periods between time spent in the crane-outrigger splint.

The anti-claw splint allows for activity and exercise while keeping the metacarpal joints flexed. Eventually, the anti-claw splint replaces the crane-outrigger for daily activities.
Glossary of Terms
hover over a term to go back to where it was first referenced in the text
Peripheral nerves: nerves in the body that belong to the peripheral nervous system; everything but the brain and spinal cord
Neurons: specialized cells in the nervous system that communicate via electrical and chemical signals; also known as nerve cells
Motor neuron: neuron in the central nervous system whose axons travel outside of the central nervous system to control muscles, producing movement
Sensory neuron: neuron in the central nervous system that senses sensory input and relays the information to the sensory cortex in the brain
Cell body: main part of the neuron where dendrites branch; contains organelles and the cell's nucleus
Dendrites: branches that project from the cell bodies of neurons; can inhibit or stimulate other neurons
Axon: also known as a nerve fiber; a long, slender projection of a neuron that sends impulses away from the neuron's cell body
Axon terminal: distal terminations of the branches of an axon; release chemicals
Upper motor neuron: motor neurons that originate in the motor region of the cortex; carry motor information down to the final common pathway
Lower motor neuron: are the motor neurons connecting the brainstem and spinal cord to muscle fibers
Myelin sheath: insulating layer of Schwann cells that covers the axons of motor and sensory neurons; primary function is to speed up neural impulses and protect the axon
Schwann cells: cells that maintain homeostasis in the nervous system by: insulating neurons, providing support, aiding in nerve regeneration, and destroying pathogens
Hand transplant surgery: surgery in which a hand from one human is transplanted onto another
Nerve regeneration: the process of growth and repair in the peripheral nervous system; nerves may grow at a rate of up to one millimeter per day (1 inch per month)
Wallerian degeneration: axon degeneration that occurs distal to a nerve cut or crush injury
Cortical reintegration: neural reorganization that occurs in the brain in response to hand transplantation
Primary motor cortex: primary motor area of the brain contributing to generating neural impulses that pass down the spinal cord and control the execution of movement
Primary somatosensory cortex: the main sensory receptive area for the sense of touch
Phantom limb pain: sensation that an amputated or missing limb is still attached to the body
Homunculus: term used in various fields of study to refer to any representation of a human being
Functional magnetic resonance imaging (fMRI): an MRI procedure that measures brain activity by detecting associated changes in blood flow
Transcranial magnetic stimulation (TMS): noninvasive method of measuring brain activity that uses a magnetic field to induce polarization of neurons
Post-operative splint: splint applied immediately after surgery to protect tissues and properly position the limbs during healing
Early protective motion (EPM): early movement exercises performed by a hand therapist to facilitate healing and preserve soft tissue integrity
Passive range of motion (PROM): in physical therapy, when a therapist moves the joint through the range of motion with no effort from the patient
Crane-outrigger splint: type of splint that supports bones of the forearm while protecting the extensor muscles from shortening due to a lack of use during recovery; uses a pulley system to facilitate movement of extensor muscles
Anti-claw (dorsal hood) splint: smaller splint used several months after hand transplantation surgery; blocks hyperextension of knuckle (MCP) joints